![]()
![]()
![]()
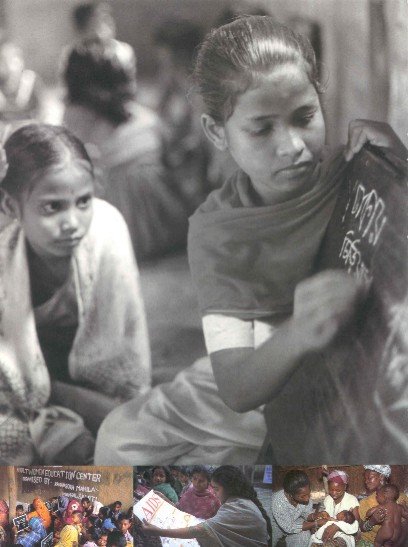
EDUCATION
HEALTH
Almost two out of every three illiterate people are women. The world's poor women are more than 100 times more likely to die of causes related to pregnancy and childbirth than women in Europe.
Our commitment to improving education and health services for women was demonstrated by the Prime Minister's pledge at the 1997 Denver Summit to double our expenditure in health, education, and clean water in Africa by the year 2000.
|
We are clear about some basic principles: · girls and women should have opportunities for personal growth, security, realisation of rights, control of fertility and health, literacy and opportunities to participate in political and economic systems... Clare Short, Secretary of State for International
Development. Speech at the UK launch of the UNDP Human Development Report, June
1997. |
Schooling
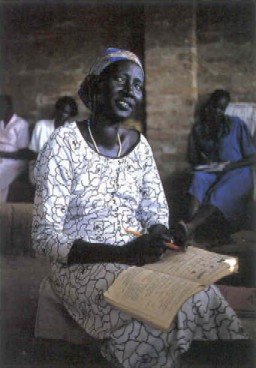
Literacy and Non-Formal Education
Recent research shows that investment in education for girls is the single most effective way to reduce poverty Even a few years of basic education empowers women to have smaller and healthier families and enjoy a higher standard of living Educated mothers are also more likely to send their children to school, creating a virtuous cycle of education and poverty reduction.
International progress in reducing gender disparities in education has been encouraging, but there is still a long way to go.
We have helped develop new plans for education in Tanzania and Uganda These include specific targets for the greater involvement of female students and teachers Improving the participation of the wider community, particularly women, in the management of schools and the schooling process are also priorities.
Social analysis undertaken in the design phase of a new education project in Guyana showed the inextricable links for women between poverty, social exclusion, and lack of education This project now has a strong gender focus.
In Kenya, the DFID-funded Support to Primary Education (SPRED) project includes a comprehensive gender strategy. Research funded through the project has identified barriers to girls' attendance and performance at school. Gender-aware approaches have been developed to in-service teacher training and class and school management techniques A voluntary code of conduct has been agreed with local publishers and authors to eliminate gender stereotyping from reading materials.
|
Marlene is an 18-year-old mother of three, now pregnant with her fourth child. She lives with her partner and children in a small one-room wood and zinc building with a sand floor. Their home is not serviced by water or electricity and has no sanitation... Marlene dropped out of high school when she became pregnant in the third year. Her eldest daughter is in the first year of nursery school. Her partner works mining for gold in the interior, which takes him away for periods of up to six weeks. Marlene is left to care for the children and has little support beyond that provided by neighbours... Jean is in her thirties. She has one child by her present partner and two other children from a previous relationship. Like Marlene, she and her family live in a one-room shack, with no utilities. Her partner also works in the bush and is away for long periods. When she is alone she often feels insecure, as people often bang on the windows at night. There is a high incidence of rape in the area, particularly when girls go to fetch water from the standpipe by the main road. Some days she and her children go without meals... Jean's daughter is now of nursery school age but is not attending because she cannot afford the uniform, shoes or snacks. Social Appraisal, Guyana Education Access Project, April
1998 |
In India, DFID is supporting the District Primary Education Programme in Andhra Pradesh and West Bengal This is part of a nationwide programme to improve quality, access, enrolment and retention in primary education, particularly for girls, especially those from disadvantaged and vulnerable groups such as scheduled tribes, scheduled castes, religious minorities, working children, and migrants
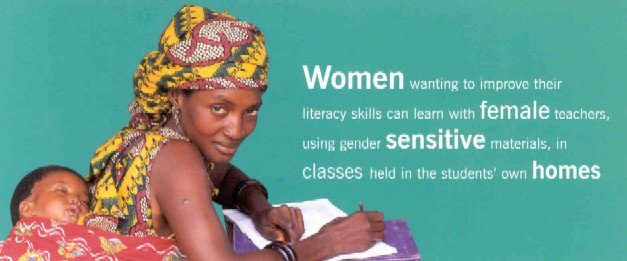
As well as supporting improvements in schools, we are also addressing the special learning needs of women and girls who have never been to school or dropped out at an early age. In Egypt, for example, we are helping to improve the skills of rural literacy teachers who are working with women of all ages who have never been to school. Women wanting to improve their literacy skills can learn with female teachers, using gender sensitive materials, in classes held in the students' own homes. The project has also supported national television programmes which emphasise women's role in development.
We are part of a multi-donor consortium supporting the Bangladesh Rural Advancement Committee (BRAC), which has developed an education programme with significant benefits for young girls. The project supports 34,000 low-cost single classroom schools. Each class enrols 33 children, 70% of whom are girls, and provides a three-year programme after which the children transfer to the formal system to complete their primary schooling.
|
The Government's White Paper, Eliminating World Poverty: A Challenge for the 21st Century states that we will focus our support on the fundamental elements of an effective education system: access, quality, retention and equity: · Access - for girls as well as boys, rich or poor, rural or urban, and those in socially or ethnically disadvantaged communities |
Children by Choice
Maternal Mortality
Sexual Health...
...Including for Young People
Involving Women
Female Genital Mutilation
DFID is one of the world's leading donors in the health sector. Our spending on health has more than doubled in the 1990s.
Our priorities include promoting children by choice and improving sexual and reproductive health. We are also addressing maternal mortality and other health risks associated with pregnancy and childbirth.
The 1994 Cairo Conference on Population and Development recognised the direct link between health and women's empowerment, and we seek to carry this forward in our work.
We have made an important contribution to slowing the rate of world population growth and creating opportunities for women to choose when to have children and the family size they want.
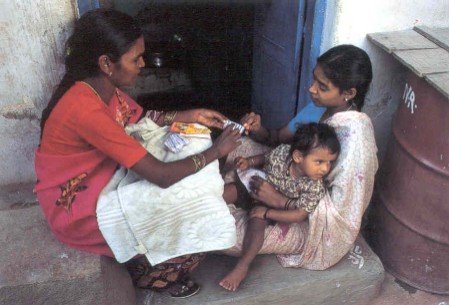
Improving the availability of contraceptives is essential to this work. We work with governments, NGOs and other organisations, and support the subsidised social marketing of condoms and other contraceptives, in Cambodia, India, Latvia, Nigeria, Pakistan, Russia, South Africa, Zambia and Zimbabwe.
A key target for the 2Ist century is to reduce maternal mortality rates by three-quarters. This is a huge challenge. DFID's four-point plan for safer motherhood ensures that:
· women have sufficient information to make sound decisions about their health before and during pregnancy;We are supporting work to implement this plan, with new initiatives now underway in Kenya, Malawi, and Nepal.· good quality services are provided and accessible at all times;
· women in need and their carers can call for help and access services when necessary;
· the safety of motherhood is properly monitored and appropriate action taken as a result of the information obtained.
|
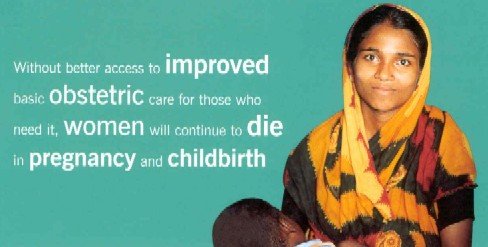
Nowhere are the obstacles faced by women to health - and the inequalities faced by poor women -revealed more starkly than in the figures for maternal mortality. The tragedy and indecency is that we know the major causes of maternal mortality, and the kind of care that pregnant women need when things go wrong. Without better access to improved basic obstetric care for those who need it, women will continue to die in pregnancy and childbirth. We must do better. These are not principally matters of science. They are matter of political and moral choice and will Clare Short, Secretary of State for International
Development. Speech on World Population Day, 1997. |
Better sexual health is a priority Women are especially vulnerable to infection which often goes unnoticed until serious damage has been done HIV/AIDS is a particular concern, both because of the devastating effects it has on individuals and communities and because of the disproportionate burden of care which falls on women We support programmes which improve access to quality basic services, and community-based campaigns to promote safer sex to help empower women and girls to reject unwanted sexual attention
Ground breaking DFID-funded research in East Africa has shown that early and thorough treatment of sexually transmitted infections can reduce the incidence of HIV infection by as much as 40%.
In many parts of the world, young people are denied access to sexual health services, despite the fact that every year one in 20 young people world-wide contracts a sexually transmitted infection More than 60% of new HIV infections are in young people aged between I5 and 24, the majority of whom are girls
DFID's strategy is to support initiatives to
· improve young people's access to information about sex and sexuality,We aim to provide information to young people in a language and style they can easily understand.· help develop social skills and gender awareness (particularly among young men) to enable them to be more responsible in sexual relationships and develop confidence, self-respect, and respect for others; and
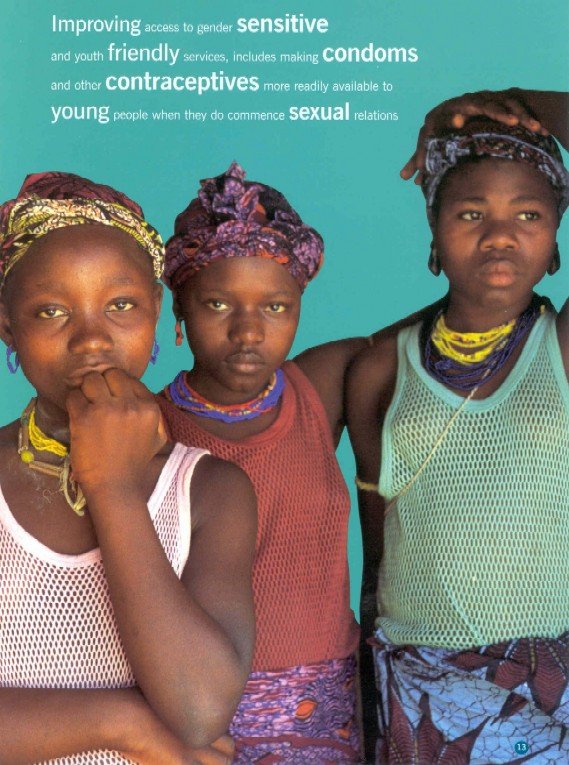
· improve access to gender sensitive, and youth friendly services, including making condoms and other contraceptives more readily available to young people when they do commence sexual relations
Making health services more responsive to women's needs is one of our key aims. In East Africa and Latin America, guidelines have been developed for involving women in assessing the quality of reproductive health services and using the findings to make improvements.
A health promotion pilot project in The Gambia is just one example of our work to help end the practice of female genital mutilation. We are also supporting the World Health Organisation (WHO) in its efforts to develop policy and coordinate a better international response to the problem.
![]()
![]()
![]()